It has been a while since I have written – almost two years. And what a two years it has been!
Given the amount of media coverage on both sides of the approaching federal referendum on an Indigenous Voice to Parliament, in mid-January I sat down and wrote an essay on how, as a regular church goer, I might consider my voice in this significant time in Australia’s history.
If you are interested to read it, the essay is here.
I am looking forward, with timidity, to reading and reviewing the final report from the Royal Commission into Aged Care Quality and Safety.
As you might recall, I retired on 1 November 2019 on grounds of ill following an almost 40 year career in aged care management and leadership, and three Chief Executive Officer positions totaling more than twenty years.
In my view, whilst the funding is the highest it has ever been, the care provided within that funding is at least as poor as that provided in the mid 1980s which prompted the (Senator) Giles review into nursing homes. In my view, based on a competent clinical assessment of their health and multiple morbidities with which most seniors approach care services for support, our current aged care system, whether for residential and/or home based care, is unable to guarantee that each care recipient will receive the care they need, let alone want.
The aged care sector needs MORE:
More funding for care;
More staffing for care;
Mandated minimum staff mix ratios expressed as a required hours and minutes per day based on the appropriate assessment of clinical and support needs of residents and home care clients;
More training for staff;
More regulatory oversight by an assessment/audit authority (with teeth) that can fine and disqualify company directors and/or officers for breaches of regulatory compliance;
More transparency about where the $ billions are spent each year, particularly in profits and shareholder dividends (away from care);
More input from feet on the ground consumer advocacy groups;
More transparency and exposure of inappropriate care that endangers aged care recipients’ health, well-being, and safety;
More initiatives for care and accommodation services for –
People living with dementia; and
Older, frail (mainly) women at risk of homelessness, but reliant on a pension only, due to lack of sufficient retirement funds to support private accommodation.
More high care community aged care packages made urgently available in communities where they are needed, along with a contemporaneous moratorium on the issuing of residential aged care places in those communities so that our dependence on residential aged care is lowered; and
More research into financing models making use of occupational superannuation or similar insurance funding, for example, making use of a wage rise incentive for more superannuation, but the relevant contributions set aside with regulation for later use in instances of aged care and/or disability care services and related purposes.
Mine is a long list, but I think not unreasonable. And I have likely omitted to mention some that I should have included.
My own work on minimum staffing requirements (here) back in 2018 suggests about an additional $6 billion to have a workforce sufficient in number and training to appropriately care for our most frail if elders. Today many residential aged care services do not even have a registered nurse on duty 24 X 7, with perhaps only one or two staff for 100 or more residents. In my view this is a shameful outcome of what has been, in hindsight, some thirty-five years of failure of what promised to be an innovative Aged Care Act in Australia.
There is going to be tough times ahead for all involved and the final report/s are likely going to make for difficult reading. But they must be both read and acted upon.
The question is, will the Australia Government have the appetite and conviction to introduce rights based changes in care for our elderly. Or will older Australians face an uncertain future with respect to their care needs in later life?
UPDATED to include responses to questions I asked of the Australian Government Department of Health’s COVID-19 Vaccine Team
Its been a little while and I haven’t been that well.
I wrote an essay on the weekend of 12, 13, and 14 February 2021 about use of vaccines by Christians (and more generally, people of faith). The essay focuses on how we might best respond to some of the new COVID vaccines that have a development and indeed a testing basis in foetal cell lines, descendant from decades old aborted human foetal cells.
This can be a complex area of morality and bioethics for people of faith. The essay is not a short read, but I do hope you find it both informative and helpful for yourself, and perhaps even your own faith community. If you appreciate the work, please feel free to share and discuss within your community.
Oh, and there is a couple of questions to which I could not (yet) give a more complete response. I have asked the Australian Government’s COVID resource team to provide a considered view. I hope that they come through on this.
Contemporaneously I have been compiling a library of similar indicators that I believe will be useful in our overall aged care sector. There are some differences between my work, the report provided to the Royal Commission, the Australian Government’s mandatory reportable quality indicators,[2] indicators used by the Victorian Government in its State managed residential aged care facilities,[3] and an international source of over 90 indicators[4] that I have used. The main differences are that where most of those other sources focus on quality of care and safety, and quality of life indicators, I have also built in indicators around, quality of assets, equipment, and supplies, and organisational governance.
Courtesy Michal Mrozek – https://unsplash.com
This is not to suggest that my library of currently 194 indicators is complete. On the contrary, the ROSA report prepared for the Royal Commission “A total of 305 quality and safety indicators for residential aged care were identified”.[5] At some point a limit is reached as to what quantity is manageable to be measured, recorded; and if made mandatory, reported.
things never really do stay the same – we can and will adapt to the new normal
Toward the end of my previous essay I indicated that I would focus on KPIs in this Blog Piece. I will get to that next time – I feel it important to make some commentary on the impact that COVID-19 is having on the services of our aged care colleagues in Victoria. This week saw a specific focus by the Royal Commission into Aged Care Quality and Safety on the management of, and planning for, COVID-19 outbreaks in New South Wales and Victoria. The following dot points are some of a tweet thread I made on Saturday morning summarising my take on the week’s evidence:
Surely what we are seeing is just the unintended consequence of an uncontrollable pandemic virus? No! Early “antidotes” to this situation could have been planned as proactive mitigation action;
In February 2020 we could already see the impact of COVID around the world. When Dorothy Henderson Lodge and Newmarch House hit in March and April in NSW, who indeed was occupying the empty hospital beds? Why not admit COVID+ residents;
But it is more than that. For almost two decades there has been calls for regulated 24X7 RN coverage and mandated staff mix and supply. The benefit to care quality/safety has been demonstrated;
Others have relentlessly advocated for greater transparency in reporting of complaints and poor quality outcomes, knowing that incremental improvement can lead to better care outcomes;
Others have lobbied for increased funding for provision of services based on wage inequality for care staff vs the health care sector. Aged care lags behind Health as a poor cousin – again negatively impacting care;
We are left with residents dying and families in despair. Tragic outcomes from known, foreseeable, and preventable failure of over 20 years of aged care policy and funding.
Committing to the formation of strategy, developing that strategy and communicating it are significant responsibilities of any board.
How best can the developed strategy be measured, reviewed, and managed?
I will leave the measurement of strategy performance for the third in this series of short essays. This short essay focuses on the board’s management of its strategy through the Chief Executive (howsoever titled).
There is nothing that quite replaces the annual board get-away for deep, focused strategic thinking about its role, its responsibilities, and the organisation in which its fiscal duties and fiduciary responsibilities are invested. These can be richly rewarding times, and if well facilitated, can bring long term, positive momentum to the board and senior management, with a renewed focus on organisationally important things to be achieved. But if your board’s last strategic thinking and planning session was, say, in November 2019, you know now that the world has almost completely changed within one calendar quarter.
Your board no doubt meets several times each year. But do you meet to drive an Agenda to get the business done or are you meeting to drive a transformational and winning organisational culture? There is a world of difference between these two outcomes. Without detracting from the value of still getting away for an annual, thorough review of strategy, there are useful alternatives that make more frequently inclusive focus on strategy at regular “any time”[1] board meetings, and more formally on a periodic basis throughout any given year. Whether conscious or unconscious, you and your board drive the culture of the organisation in how you use the opportunities of your governance meetings.
Essentially there can be three types of meetings in which strategy can be given a dedicated place on your board agenda for its appropriate diligent review:
The Greek word σκέφτομαι (skéftomai – thinking) has the sense of contemplation, that is, more than just thinking as in this familiar image below.[1] More like thinking with care or weighing up the impact of thoughts. From this word we get the word skéfto.
Over the years I have been on boards where strategy, its measurement and monitoring have been left to the CEO to lead; and where strategy was not a matter that was on the board agenda in regular (monthly) meetings.
I encourage us all to seriously think about how we can amend agendas to include strategy as a priority item on each board meeting.
Boards can learn how to ask questions of the executive team and management around matters rolled into their Strategic Plan. For example, if you have ten overarching objectives in your current strategic planning document, and your board meets ten or eleven times each year, you could consider a well thought out sixty minutes of discussion around each of these high level objectives at each Board meeting, and the entire Plan would be discussed throughout the year. To provide time for input from the CEO and executive team, even if the Board were to conduct that review of each item in the Plan over a two month period, the entire plan could be thoroughly discussed and re-invigorated every two years. This does not detract of course from the value of a formal annual Strategic Planning review.
However, too often we lay responsibility (blame) at the feet of the CEO and executive team if strategy is not achieved or seems to waver along the path the organisation sets. This is most unfair if the board itself is not taking care of the primary responsibilities of monitoring and oversight of the organisation’s strategy and strategic plan for which it is responsible.
In his well-known text on governance, Tricker describes the basic board functions[2] working through management as:
Just the other day on 15 June 2020 we honoured World Elder Abuse Awareness Day, a day that highlights elder abuse in all of the forms it manifests itself.
Australia has had its own recent and continuing struggles with prevention of spread of COVID-19, and I feel proud to be both an Australian and supporter of most of our aged care providers in how they have managed well in these complex times. As we know, our experience has not been shared with numerous other western nations.
Just one week ago, the Kaiser Family Foundation (“KFF”) released the following summary of data around prevalence and mortality rates due to COVID-19 in USA long term care facilities – for ease of discussion, let’s call them all nursing homes. Remembering that the population of the United States of America is about 13 times that of Australia:
As at 11 June 2020, 44 States reported 9,192 current cases of COVID-19 infection in nursing homes;
Collectively, 43 States have reported a total of 230,776 COVID-19 cases in nursing homes;
From 40 States, there has been a combined total of 45,833 COVID-19 related deaths reported in nursing homes;
From 43 States, nursing home facility COVID-19 cases represent an average 15% of the States’ total cases reported;
From 41 States, COVID-19 related deaths represent 45% of total States’ deaths.[1]
At the start of May 2020, I proposed a way in which the (residential) aged care sector might reconsider its apparent very widespread lockdown of facilities and prevention of family members visiting with loved ones in care. Various alternates of “window visits” etc had been quite successfully trialled by some providers, but they fail, for example, where a residential care facility is in a multi storey complex, with all residential living contained at above ground floor level.
There is no doubt that aged care providers have been caught in a bind with the onset of the COVID-19 pandemic. Can they have visitors at all, or on a very strict basis? What is the best guidance? Hospitals have become focused on well controlled prevention strategies – so much so that emergency department traffic has significantly slowed during this pandemic, and only now beginning to return to normal frenetic activity.
Both in hospitals, and in longer term care settings the notion of visits – human touch – in these pandemic times has been a much debated phenomenon. As a species, humanity craves touch contact with those dear to us – particularly when we are ill and so frail that we are facing death, no matter how imminent. This certainly affects the older person in care, as well as family and friends who wish to provide the touch of comfort as much as the words of caring love, concern, and, in a final sense, farewell to this life.
I am not sure how you have been managing your time during these past seven weeks. Because I am now “semi-retired”, I have taken the opportunity to read and refresh my earlier learnings over the past almost forty years on leadership, management, and strategy, while focusing on completing some studies in executive and leadership coaching.
What has struck me is that in this time of turbulent change, particularly in human services delivery right now where the impact of COVID-19 is taking its toll, is that many theories about leadership, management, strategy, and human resources management, actually have not changed, and likely do not need to. Sometimes the “old” fundamentals are as reliable as granite …
In his now famous, and dated article, Henry Mintzberg defined as a plan, ploy, pattern, position or perspective (Mintzberg, 1987, The Strategy Concept I: Five Ps For Strategy). Mintzberg described:
Stop the world – I want to get off is the title of a musical created in the 1960s.
Some 55 years later as we
become globally enmeshed in a pandemic the like of which none of us has
experienced before, one could be forgiven for wanting to shout those words from
the roof tops.
I don’t need to remind you
of the enormity of the task ahead of every organisation in every industry
sector – particularly those in a sector I am so fond of and have given over
half of my career to. I won’t belabour the size of the task ahead of
you. But I do want to ask the rhetorical questions in this group – are we
doing enough in our aged care sector to make an impact?
For providers – if you could get hold of adequate supplies of personal
protective clothing and equipment, are you considering gloving, gowning, and
masking all your front-line care staff? Are you having a skilled
Registered Nurse meet and greet every visitor and taking a temperature prior to
allowing a visitor, contractor, family member, Aged Care Quality and Safety
Commission staff member enter the facility?
For the
Australian government – Department of
Health and Aged Care Quality and Safety Commission – have you increased the
ACFI rate per resident per day, or introduced a coronavirus supplement to cover
the cost of additional medical supplies, staffing supplies, and loss of revenue
when facilities empty due to untimely death of residents? Have you
considered the financial risk and impact of failure of the RAD scheme?
This is likely a longer piece than usual, but I think important as we all consider the place of leadership mid-way through the term of appointment of the Royal Commission into Aged Care Quality and Safety.
I have been asked many times over the years I have served as a CEO, to define leadership. There are of course quotes such as “It is an art, rather than a science”. Or “You can tell if you are a leader when there is someone following behind you”. What seems to be true is that you are not born to be a leader, and leadership is not achieved from a one day development training session. However, we can grow as leaders every day – and indeed we must. And leadership is about people, whilst management is about tasks and things.
But even those small truisms above do not do justice to this
thing called leadership. Most of us can
likely recall our own examples of where we have experienced poor, or
ineffective leadership. We may even now
be wincing as we read, recognising our own lack of skills in a leadership role
at some time in the past. We can also
likely recall and acknowledge some fine experience of leadership that was such
a joy to be party to.
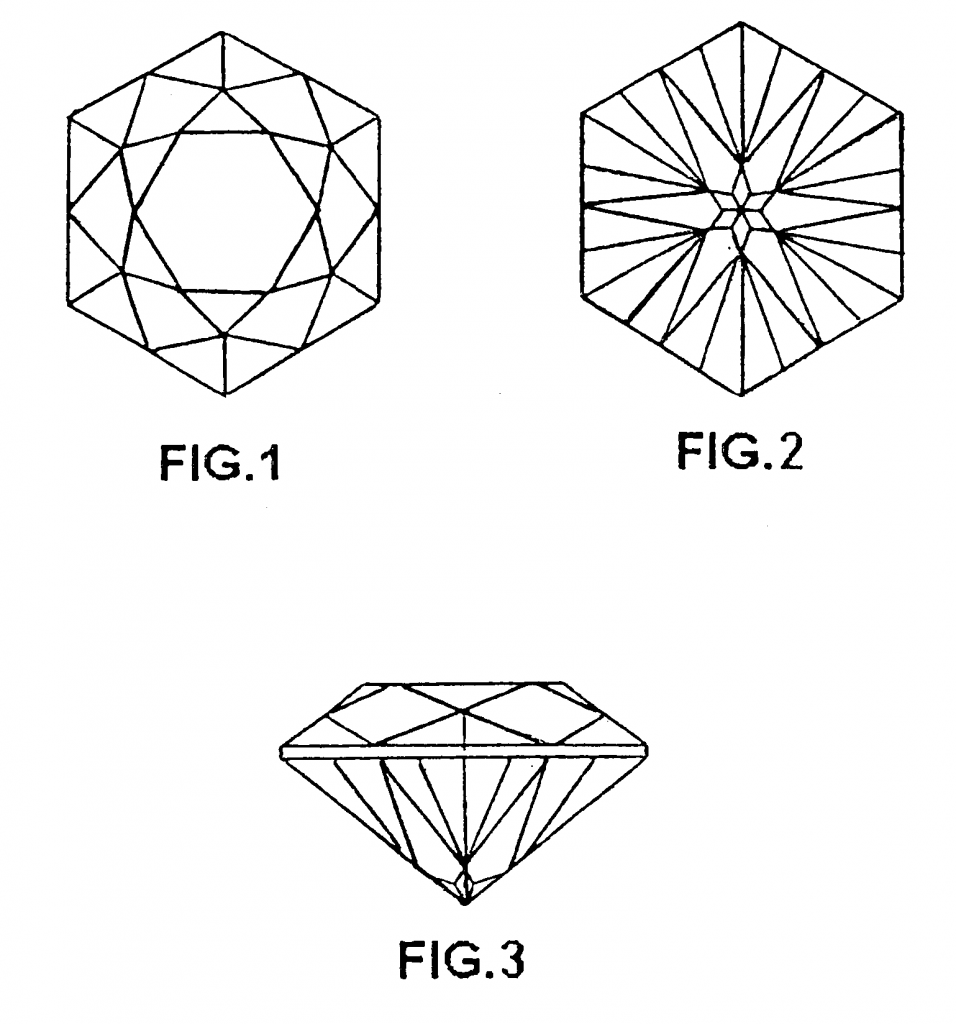
Good leadership is a thing of beauty to experience. Much like a diamond. A diamond has so many qualities and when cut well, is a thing of beauty to behold. It is hardly surprising that “diamonds are a girl’s best friend”. As the following picture shows, even a so called six sided diamond has much more to offer than the “simple” six sided cuts.
So it is with leadership.
I provide below just six sides, or attributes, of leadership that I believe if practiced (well) every day will not only assist us to be better performing leaders but will drive better performance in our organisations. I am certain we can all accept that leadership is more complex than these six, but these are a sound foundation. The attributes are provided in alphabetical order only for convenience:
No matter where and how we are involved in our Australian aged care sector, 2019 was a tough year. The sector ended 2019 with one word ringing in our ears – Neglect – being the title of the Interim Report from the Royal Commission into Aged Care Quality and Safety. What a tough end to 2019!
How do we emerge from 2019 into a brighter and stronger 2020
given that the Royal Commission continues to march on? How do we turn Neglect into
respect and rise above the negative views of all that 2019 revealed about our
sector?
I suggest that we should at least consider the following seven factors:
The following link points to the substantive comments I made in a recent submission to the Royal Commission on Aged Care Quality and Safety. As a very recently retired Chief Executive in the aged care sector, with some 37 years of continual involvement in aged care related matters, I feel I can comfortably comment upon my own research into matters around minimum levels of staff. Additionally, and importantly how, I believe, the aged care sector has been left in a quandary as to how best to navigate through these troubled times due to funding constraints placed on (at least) the residential aged care.
I have read with interest late last week the very freshly released Royal Commission research paper (1) into aged care staffing requirements, and the shortfall in funding needed to raise the staffing mix and levels to appropriately care for the average residential aged care service consumer.
The following excerpt from the recommendations paints a picture of what residents, families, advocates, and indeed some providers have been saying for some time – the level of service provision (staffing) in residential aged care in Australia is substandard.
My conclusion is that because that level of provision is so strongly associated with the operating funding mechanism, the funding mechanism for care is equally substandard:
“more than half (57.6%) of Australian residents receive care in aged care homes that have unacceptable levels of staffing (1 and 2 stars).
To bring staffing levels up to 3 stars would require an increase of 37.3% more staff hours in those facilities. This translates into an additional of 20% in total care staff hours across Australia.
We have not limited our analysis to determining the additional resources required to bring facilities up to an acceptable level. We have also provided an indication of the additional resource requirements that are required to deliver staffing levels consistent with good practice and best practice care.
For all residents to receive at least 4 stars (what we consider good practice) requires an overall increase of 37.2% in total care staffing while 5 stars (best practice) care would require an overall increase of 49.4% in total care staffing.” (2)
As you are probably well aware, I am the CEO of Braemar Presbyterian Care (“Braemar”). To put our services into perspective, since I joined Braemar in March 2017 we have been increasing hours per resident per day to a level that is close to the current national average as recorded by the StewartBrown benchmarking service (3) reporting. And, as far as is reasonable, we have been improving our subsidy income to match the staffing. But that recurrent income is not enough.
According to this research paper, prepared for the Royal Commission into Aged Care Quality and Safety, less than 3 star level of staffing is unacceptable, while a 4 star staffing is good practice, and 5 star staffing is best practice. Yet 57.6% of residents receive less than 3 star (unacceptable) staffing and only 1.4% receive best practice staffing.
How is this translated into the care of our elders?
Over the past several years I have written often on how much funding I believe the aged care sector has been short-changed by a range of political and bureaucratic decisions over. Aged care funding is not adequate to meet the health care needs of Australia’s frail elderly, vulnerable, care recipients. My comments apply across residential aged care funding and home/community care package funding alike. You can review some of my previous articles in the footnotes below. [1] [2]
Patricia Sparrow, Chief Executive of the not-profit aged care peak body Aged and Community Services Australia (ACSA), commentating recently on home care packages, lamented the lack of preparedness and capability of our aged care system, saying “Until we see adequate long-term planning for the structural and funding issues, Australia won’t be able to fully address the needs of older Australians”.[3] Sean Rooney, Chief Executive of Leading Aged Services Australia, similarly recently commented that the “aged care system needs adequate funding to be sustainable and meet the needs of seniors” and called for an additional $3 billion to “improve the viability of the sector”.[4]
Just this week I was briefed about the outcomes of a very recent Faster Horses Inside Aged Care Report (2019) of perceptions around aged care in Australia. I recommend this review to all readers of this blog. Reviewing response from over 1,500 people from a cross section of metropolitan centres, the response to two specific questions piqued my interest.
I am going to assume that most people reading this article will be aware that there is currently a Royal Commission reviewing matters of Quality and Safety in Aged Care. Among other things, that Commission is inquiring into matters where poor and substandard care have been provided to residents in residential aged care and to care recipients in home and community-based care.
Where there have been findings of substandard care, all providers in the aged care sector should stand resolutely with care recipients and be highly critical of the events that took place to permit such poor care being delivered. However, without wanting to escape from the responsibility of being a provider of aged care I do want to highlight again the dilemma that providers find themselves in desiring to provide the best care that they can.
One of the threads arising through the Royal Commission Hearings, and for some time prior to the Commission commencing has been a call for a higher staff ratio in care services being delivered.
Braemar Presbyterian Care is
offering a free community event for local people of Perth, who are interested
in learning more about palliative care.
The team have developed a Living
with Dignity, Dying in Comfort information evening, which
will take place on 22 May from 5:30PM at Braemar House, located at 10 Windsor
Road, East Fremantle.
I
spoke recently with our Professional Standards, Quality and Risk Specialist,
Bernadette Samura, who has a lot of experience in this area – having previously
managed Braemar House.
Bernadette was quick to point out
that palliative care is far more than just end-of-life care, and that it is
essential to challenge the myths and stigmas around palliative care. ‘We want
people to openly discuss it as a normal part of their future planning,’ she
told me. It is Braemar’s desire to ensure everyone involved in this quality of
life process is very much part of the care and friendship philosophy that can
add so much to quality of life.
The
evening involves a keynote presentation from Bethesda Hospital’s Clinical Nurse
Manager, Ed Gaudion, as well as exhibits showcasing various care approaches. It
is a free event, and is open to members of the community, their families with
loved ones in care facilities, those planning to relocate to residential aged
care, as well as anyone keen to learn more about palliative care.
Hope to see you there,
Wayne.
Note: The Living with Dignity, Dying in Comfort information
evening will take place on Wednesday 22 May at Braemar House in East Fremantle,
from 5:30-7PM. Coffee and light refreshments will be provided. Anyone
interested in attending this session can find out more details by contacting 08
6279 3654
In Holy Week, the week leading up to Easter, and particularly Resurrection Sunday, there are a number of things that different parts of the Christian faith celebrate.
I am from an evangelical Baptist tradition. Our Services over this important time of the year usually were solely around a reasonably solemn Good Friday morning service and then a celebration service on Easter Sunday morning. Of course the week leading up to Easter we have, among others, such things as Palm Sunday, the remembrance of the raising of Lazarus from death, Jesus cursing the fig tree at Bethany, and Jesus sharing a “Last Supper” with His disciples.
Other than for the Last Supper, until recently I had paid little attention to the events of Easter Thursday evening. Over the past ten years, we became familiar at our local church with a Service of Shadows – a Tenebrae Service – where darkness descends on the congregation following the extinguishment of a number of candles, all set around specific Scripture passages describing Jesus’ final few hours.
Easter Thursday, or Maundy Thursday, has become something special to me. But strangely it is the word “Maundy” that has caused me to rethink. The word has its roots in Latin and comes from the word “mandatum”, from which we get “mandate”. It means “command” or “commandment”. So, what commandment is this word “maundy” referring to then?
In John’s Gospel we have a few chapters describing the Last Supper and the washing of the disciples’ feet, leading to the crucifixion of and resurrection of Jesus. Indeed, approximately one third of the entire Gospel of John is dedicated to the last two weeks of Jesus’ life, death, and resurrection. But it is in John 13:34-35 that Jesus says “A new commandment I give you: Love one another. As I have loved you so you must love one another. By this all men will know that you are my disciples, if you love one another.” Three words, a commandment, that would do us, and the entire world well to remember – “Love one another”!
After all, and contrary to popular belief and practice, Easter is not about chocolate and hot cross buns. It is about one sacrifice for the world, given in love. So love one another!
Have a safe and happy Easter. If you are travelling, please remain vigilant. Enjoy your break. If you are working – thank you for your continued service.
If you have the opportunity, why not stop into a church for an Easter Service and join with others as we celebrate this hugely significant time of the year in our faith journey and annual calendar?
A former Australian of the Year recently said, “The standard
you walk by is the standard you accept”. In aged care, we are entrusted to care
for and support some of the most vulnerable in our community. It is my belief
that in this industry, we must only accept the highest standard.
While I am proud of the quality of care we deliver at
Braemar, I am a strong believer in creating an environment that encourages
constant improvement. We want to be open and accountable in all we do.
To ensure that everyone associated with our organisation is
able to have their voice heard; about any issues that cause them concern; we
have introduced a new service called Your Call.
Your Call is an independent, third-party reporting service
which allows residents, family members and staff to report any matters of
concern in relation to the care and services we provide.
Sometimes, for various reasons, we might feel uncertain or
uncomfortable about directly raising an issue or reporting something we have
seen.
It is my hope that this new service will provide those
living in care, as well as their families, friends and staff, with an
environment in which to raise any concern – no matter how big or small.
Reports to Your Call can be made anonymously. Those lodging
a report can do so by phone or online – 24 hours a day. All reports are
forwarded directly to me for immediate consideration and action.
Contact details for Your Call have been distributed
throughout Braemar’s facilities. This has been done via the installation of
large posters; while printed information and updates are being made available.
This service is available to all our staff, residents and
family members and friends. It is essential that as aged care providers we
ensure we are transparent in all we do.
I want to ensure we hear from you if you have any concerns.
I am excited to see Braemar lead by example in this area.
Many years ago, I spent one Christmas time away from family and stayed with friends in the Great Southern area of Western Australia. Their father had died when they were both quite young.
View this greeting as a video.
As boys, these brothers became the men in the family and over time built up their farming property to be a successful enterprise. They were both good, honest, hardworking men, who also were faithful in their Christian belief.
I could certainly talk with them about harvest time, how the wheat, barley,and oats grew, why back then one had to wait until a little later in the morning to start up the header and get out and cut into the crop. But talking about personal things was difficult for them – they were just quiet guys who had some really good things to say, but just didn’t much like speaking it out.
There is this man talked about in the Bible who really had a huge impact about all we believe and practice at Christmas time, but of whom, from Scripture, we never hear a spoken word. We hear from Mary, the mother of Jesus, in the first chapter of Luke’s Gospel. Tradition has called Mary’s Song the Magnificat. We hear from Elizabeth, the mother of John the Baptist, and (eventually) from Zechariah, John’s father.
But we don’t ever read a recorded word that was spoken by Joseph. Oh,we read of his at least three dream encounters with an angel, or God Himself –first with a message to take Mary as his wife and raise Jesus as his father;the second to flee from Israel and travel to Egypt – an historic refugee journey – and third; to return to Israel because it was now safe to doso. Given the cultural and societal significance of all of the above,Joseph was a very courageous man. The strong silent type if you will. A lowly carpenter, from one of the lowliest places in the whole of Israel, at that time overrun by the Roman Empire, and “ruled” by a king who was a Roman puppet. Joseph did not have to do this, but he felt so led by God that he could not avoid the challenge set before him.
Just a day or so ago I read this social media post: “Sometimes God will puta Goliath in your life, for you to find the David within you.” I am sure that Joseph will have wondered something like “You want me to do what exactly?”,or “Why me?”, but he did. We just don’t ever hear his thoughts and words expressed.
There are some significant challenges in the year ahead for our aged care work. The looming Goliath is of course the Royal Commission into AgedCare Quality and Safety. You may already feel quite uneasy about what that is likely to reveal and how we will get through this. We will – no matter how much we are required to provide, and even to share with the Australian public – we will get through this.
My concern for each of you though is that even if your voice does not godown in any formal recorded historical moment, if you have any concerns about your wellbeing through this next twelve months, speak up. We want to also care for you. If you need at any time to share any concern about our behaviour that is both unbecoming, and contrary to our desire to provide a dignified life to our residents, then please share that with us too, so that we all be a “David” and improve how we provide our services.
Folks, I pray and hope that your 2018 Christmas brings you much joy, peace,and blessing, and that you have at least some time to reflect of the enormity of the coming of Jesus into the world – not to destroy the world, but to saveit!God bless you all – and Happy Christmas!
These days I only read the newspaper on the weekend. My favourite is still The Weekend Australian. It often has thought provoking articles, and occasionally some fodder upon which one can reflect from an aged care sector perspective.
The December 8-9, 2018 edition is just one of those occasions.
On page 2, there is an article bemoaning the recent year upon year increase in private health insurance premium rates. The article reports that ‘Health Minister Greg Hunt … expected to approve an industry average below 3.95 per cent … the lowest since 2001.’ It also includes commentary about the anticipated significantly lower rate increase out to 2022 promised by the current Federal Opposition.
According to Australian Prudential Regulation Authority (APRA) figures cited by The Weekend Australian, the industry weighted average premium increases approved by the Minister for Health since 2015 are as follows:
I understand the impact of high levels of private health insurance premiums, that seem reachable by those who for whatever reason determine them to be affordable. What is more, in contrast to aged care funding, the payment of insurance premiums does not come from the Government purse, but rather from individuals who have determined their affordability.
I find this article useful, if only because for almost the past twenty years I have been monitoring Health Ministers making similar approvals for health insurance premium increases yet at the same time, as the senior Minister over the aged care portfolio, makingstarkly lower indexation for payments for recipients of care or, more indirectly, to the providers of care to aged care recipients.
The comparison of funding increases made to aged care providers through the various indexations against several alternate indicia is shown below:
The chart above clearly shows that whilst aged care funding indexation has indeed kept fairly much in line with CPI, it has failed to keep close to Work Price Index (“WPI”), Average Weekly Earnings (“AWE”), and the greatest gap is between aged care funding and private health insurance premiums.
I will be among the first to say that additional funds are not always the determinant of better quality. Yet the absence of an equitable funding methodology in residential aged care since 1997, and growing concern about insufficient supply of places in community based aged care since February 2017, seems obvious.
Inclusive of some $1.7 billion removed from forward funds in 2015 and 2016, there is a clear pattern of diminishing Government expenditure in aged care over the past twenty years to a point where it is highly unlikely that even courageous and good providers of care will be able to sustain their service provision without a sizeable injection of funding.
It has been just three days since the Federal Standing Committee on Health, Aged Care and Sport recommended support for the Aged Care Amendment (Staffing Ratio Disclosure) Bill 2018.
I support the recommendation that aged care providers disclose their staffing ratios. However, it would be unreasonable to expect that providers will be able to achieve a reasonable staff ratio without an immediate and substantial injection of funds – albeit with reporting requirements.
Perhaps the Royal Commission can consider this matter in their review processes into the whole aged care sector quality and safety funding and performance?
House of Representatives Standing Committee on Health Aged Care and Sport, ‘Advisory Report on the Aged Care Amendment (Staffing Ratio Disclosure) Bill 2018’ (Commonwealth of Australia, Canberra), December 2018
Sean Parnell, ‘Rise in health premiums likely lowest in decades’, The Australian (Sydney, NSW), 8 December 2018
I gathered these thoughts together the day the Royal Commission into Aged Care Quality and Safety was announced – Sunday 16 September 2018 if my memory serves me well.
This information gathering was in response to the first question of the Prime Minister when making the announcement. The question was around the alleged $1.2 billion cuts to aged care.
Folks, I get it – there have been many cuts from both major sides of our Australian Government over a number of years. And there has been continuing growth in aged care funding based on population related indices etc. But what is galling around these discussions is that the major political parties and the bureaucrats seem unwilling to give simple, transparent responses to questions about these matters.
The recent Federal Senate Community Affairs Committee Hansard from 24 October 2018 make for mind numbing obfuscation around this very issue, with Opposition asking relevant questions, and Government, and Officers, all putting in their opinions, without any direct answer to what should be a simple question. This of course happens regularly at such Committees and is not confined to Aged Care. But this Australian is over it!
Why cannot our elected leaders and paid Officers answer simple questions and be held accountable for the policy and funding interventions they create into valued human service provision? We are projecting tens of thousands shortfall of residential aged care places by 2025 (ref 1) and now some 121,000 not provided with an appropriate level of community care packages short for older Australians already assessed by Government as needing community delivered aged care services. (ref 2).
Of that number, almost 57,000 had no package allocated. A discussion around the residential care funding issues can be found below. Parliamentarians prefer to support their side of the debate, but the Department of Health and Federal Parliamentary Library advice really does paint a helpful and insightful picture into this matter of “funding cuts”.
I shall leave it to you to decide. But if you were to ask me, a return to the residential aged care sector of the $1.2 billion in ACFI funding cuts, along with a requirement for providers to sign off on their direct care staff ratios, would provide, on average, an immediate return to a ratio of 3.2 Hours per Resident per Day (“HRPD”), and begin a move to the 4.3 (or from my research, 4.2) HRPD as soon as possible.
ACFI – December 2015 MYEFO (might be a repeat of the May 2015 budget papers) – https://manad.com.au/aged-care-cut-in-mid-year-economic-and-fiscal-outlook-myefo/ The following is on an Australian Parliamentary Library page and really cannot be disputed. The page is at – https://www.aph.gov.au/About_Parliament/Parliamentary_Departments/Parliamentary_Librar y/FlagPost/2017/March/Residential_aged_care_funding
“Recent changes:
ACFI subsidy expenditure has been growing more quickly than expected. The Australian Government believes the unexpected growth in claims cannot be explained by an increase in the frailty of residents, although many in the industry disagree. In order to rein in expenditure, around $1.7 billion in savings over four years were included in the Mid-Year Economic and Fiscal Outlook 2015–16 (MYEFO) and the 2016–17 Budget, to be achieved through changes to ACFI scoring and subsidy indexation. Despite these savings, residential aged care expenditure was still forecast to grow at around 5.1 per cent per annum.” A summary of the impact of these two difficult measures can be found below – https://www.aph.gov.au/About_Parliament/Parliamentary_Departments/Parliamentary_Librar y/pubs/rp/BudgetReview201617/AgedCare
“Rein in expenditure.” Is that not just a euphemism for a cut to funding?
You decide. Nice chatting!
References:
Ref 1- Aged Care Financing Authority, ‘Sixth report on the Funding and Financing of the Aged Care Sector’ (Aged Care Financing Authority, 2018), 36.
Ref 2 – Department of Health, ‘HOME CARE PACKAGES PROGRAM Data Report 4th Quarter 2017 – 18’ (Department of Health, 2018), Table 7, 11.
I am a person with no clinical or “care” background. But after almost forty years in senior management and executive roles across the spectrum of health and aged care – particularly aged care – I have gathered some insights into the nature of care being provided throughout our care services.
And before I suggest anything more, let me say this – my view is that if the major hospitals around Australia – public and private – were put under the same scrutiny and regulatory framework that residential aged care services are for the quality and accreditation of services that are provided in and through them, we would see hospitals falling into sanctions.
I am of the view that we have an aged care system that is too focused on beating the regulatory compliance framework as opposed to funding and providing appropriate levels of care and support to all clients.
On the one hand I am an incredibly strong advocate of high quality services accompanied with some form of accreditation. On the other hand, I believe we have an aged care accreditation system that we can really ill afford.
It underpins inadequate funding levels that cannot provide enough resources for many providers to meet the expressed needs of care for residents. In the same way, our community aged care system is creaking because we cannot provide enough funding for the community aged care packages assessed by the Australian Government as needed by our citizens.
I hear staff all over Australia clamouring, not always for more wages, but for more pairs of hands to do the work. To do more than the system underpins…To go the extra mile… To sit for a few minutes when that is what the client really wants, and really needs… To spend time hearing what the real story is…
To quote a UK study of its Home Help services from the early 1980s – “Too much Charring and not enough Chatting”.
I could ask the question – Which provides more care, the Chatting or the Charring? Neither is necessarily more correct, but often we cannot even get to the question. The bureaucratisation of aged care is with us and the paperwork must be done at our own peril.
I have colleagues that will not (at this time) support minimum staff ratios. Quite rightly they see them as an un-affordable cost under the current funding methodology. How sad that we do not all see them as providing perhaps the single greatest opportunity right now to see a reduction in abuse, and a reduction in short cuts in care. How sad that we do not see minimum staff ratios as an opportunity to support our staff and see a visual improvement in the increased in quality of care. But implementation of minimum staff ratios will be quite costly.
I am still of the view that in Australia we have one the best aged care systems in the world. But for a range of reasons it is creaking.
Let’s all is to consider how much of a cost is there to stop, take stock, and with the next round of changes, really consider the long term impact of where we are heading and fight more intensely to protect the rights of those who are dependent upon us, the general public, for their livelihoods?
And who knows – the Royal Commission might investigate several inter services aspects around care of our elderly folks? One matter that I have discussed for the past decade is how much more proactive care we can provide in our aged care facilities, that might actually have a positive, beneficial impact on our national health and hospital care services.
In the past twenty years we have missed the opportunity to think outside the square with respect to fixing major State based hospitals. As a “cohort” of patients, frail elderly people are significant and frequent users of hospital services. Perhaps if we reviewed the aged care sector and its inherent possibilities we might find better solutions to our hospital problems.
Chatfield’s cartoon below was first published by me in December 2010 in an article containing many of the words in the commentary above. Not much has changed it seems!
So, what is the elephant in the room with aged care at the moment?
In a report released Friday 17 August 2018 that showed a recent increase in home care funding for elderly care recipients, there was a worrying trend in demand versus ability to provide that needed care.
That is, despite the growth in older people desiring home care services, the number of home care packages assigned (or available) is simply not keeping up with demand.
At 31 March 2018, according to figures only released on 17 August 2018, the queue waiting to receive a package had risen to 108,456 people. That is an increase of 3,854 on those waiting at 31 December 2017. Not only that , but just over half of all those in the queue have been assigned a package at a lower level than their needs require. Remember this is all based on the Australian Government’s own approved needs assessment, and allocation of packages.
Contemporaneously we have demographers projecting the number of residential aged care places required to be built/developed is now at about 75,000 by 2025. That is only eight years away.
The word governance may well have been used by Chaucer in 14th century England, but the phrase ‘corporate governance’ has only been commonly used since the 1980s.
Major corporate failures such as Enron, WorldCom, HIH, the dot.com crisis, the global financial crisis, and the Royal Commissions into institutional abuse of children and the banking sector, have increased governance expectations.
The community requires corporations to improve the way in which corporate governance is practiced.
That is, more is expected from companies behaving as good citizens.
Although not a legal term, ‘corporate governance’ does carry the sense of needing to be defined. It regularly arises in actions or Commissions as something lacking in practice.
Yet the concept of corporate governance has struggled to have a single definition. Early definitions were based around corporate governance being the ‘system by which companies are directed and controlled’ (Cadbury Report, 1992; King, 1994).
The Australian Stock Exchange recently broadened the scope of the concept of corporate governance to ‘the framework of rules, relationships, systems, and processes within and by which authority is exercised and controlled in corporations’.
Similarly, the G20/OECD principles discuss how the monitoring of performance against structure of organisational objectives can deliver better
governance outcomes.
I have never been a great advocate for regulated minimum staffing ratios, but prefer regulation of the things that are really important around provision of care services to the people, our care recipients. If you like, having enough of the right people at the right time, and not just to fulfil a compliance requirement around the number of pairs of hands.
In completing this Review my own views around staffing, quality of care, industrial considerations and the like have changed – for the better. It remains to be seen if those with the capacity to make an even more profound difference to improve care outcomes for frail, vulnerable, mainly elderly recipients of care – the Australian Government and Parliament – will actually choose to support those whom we serve.
Introduction
It seems that in Australia rarely a month goes by where the public is not informed of another aged care failing. There is wide spread public perception of a lack of care and low quality of life for residents within the aged care system. The call for greater regulation of minimum staffing standards and additional funds to meet them is prominent but seems to fall on deaf ears of the Australian Government.
Without residential aged care provision, residents would likely be inpatients in State based hospitals at several times the daily cost of care of a residential aged care facility. However, the proportion of funds spent on care and service provision should be acquitted on what really matters – the care of people.
I have been tracking various residential aged care data and some interesting comparison figures for two decades now since the Aged Care Act came into being in 1997.Please allow me to say right upfront – collecting relevant and appropriate data from indices can be difficult and not always truly comparable.
The data represented below is purely to make us think, and perhaps identify for providers at least, why it seems to have become so much more difficult to maintain a high quality residential aged care service today to people with more pressing multiple morbidities than ever before.
Clearly, by comparison, our funding foundation has worsened over the past twenty or so years.
Some time back during one of our regular Braemar senior leadership meetings in 2017, we decided to take the lead in protecting our residents from influenza by offering complementary flu vaccines not just for our staff and residents, but also volunteers and the families of those in our care.
This week, free vaccinations were available at Braemar Cooinda and Braemar Village, while next week we will be providing the vaccines to those at Braemar House.
Here’s the latest instalment from artist Jason Chatfiled which was used as the banner on the day.
This move predated the recently announced Government plan to mandate all aged care providers to provide free flu vaccines to their staff. It was a decision we took as we felt it was an effective way to help reduce the risk of influenza entering the aged care environment.
The idea to expand the service to families and volunteers was developed by the Braemar team under the direction of Renee Reid, General Manager of Workforce. When chatting to Renee, she expressed the team’s desire to ‘meet and exceed best practice levels to reduce the risk of our health and care professionals contracting flu or passing it onto our residents,’ which to me demonstrates a commitment to resident health and wellbeing across the organisation.
I might just be getting old, but not a year goes by that I don’t think more deeply about Easter. Don’t get me wrong, I really love Christmas, and from the perspective of being a follower of Jesus, that is obviously a very special milestone of my faith. But Easter … Easter is the cornerstone event of my relationship with Jesus Christ.
In late January and early February 2018 I had the privilege of joining the Global Conference on Integrated Care (“GCIC”) in Singapore. I am delighted to say that for me this was the most beneficial conference that I have attended since my re-connection to the aged care sector in August 2016.
Every nation represented at the Conference shared information about their significantly growing healthcare budget and rapidly ageing population. All nations have health and aged care systems that were created for a previous generation. They are not designed for the massive ageing population growth that require more and more health, social and aged care services.
As often as I remind others of the difficulties aged care providers, their workforce and clients are confronted with, I remind myself that we belong to a bigger system of health and social care provision.
Many parts of that system attract what seems to us, by comparison, to be outrageous funding. Maintenance care only in a hospital costs approximately $1,200 per day. A day of care in an intensive care unit costs $6,000 plus per day. That is not to say of course that these services are not important and desperately needed.
Despite the sector’s many recent advances, the clinical governance systems in residential aged care “are lacking”, an Australian aged care CEO will tell an international conference.
I am about to board a plane for Singapore where this week I will be speaking at the GCIC 2018 conference on integrated care.
My topic will look at where the industry may go next in its clinical governance responsibilities. I thought this was interesting to look at twenty years on from the introduction of the Aged Care Act in 1997.
I will share my full paper next week and explore some further ideas following the conference. In the Essay, I have strived to briefly describe the history of residential aged care in Australia and show how economic drivers that largely determine the funding of care may also be diminishing the clinical appropriateness of care. This can place care recipients, providers, and program funders alike potentially at risk of failure of service in financially constrained times.
Wayne Belcher (OAM) will speak at the Global Conference on Integrated Care at the start of February, where he will present an analysis of Australia’s aged care sector, two decades after the Aged Care Act (1997) was implemented.
His presentation will cover areas including the history of aged care in Australia and how it has transitioned from basic care homes to a major industry, a review of the care models currently being employed as deregulation takes effect, and a review of clinical governance.
International experts from the USA, UK, Canada and Hong Kong will be among the conference speakers, which will take place at the Resorts World Convention Centre in Singapore from 1- 3 February 2018.



















 The below is from
The below is from